UFT members received an email on August 28th alerting us to the fact that a tentative agreement has been reached with EmblemHealth/UnitedHealthcare to replace GHI-CBP, which covers about 730,000 participants when factoring in “active city workers, pre-65 retirees, and dependents.” This is obviously a matter of tremendous importance for many of us, as well as our families.
In this document, we attempt to look at what is currently known about the proposal as even handedly as possible, and within the context of the larger healthcare agreements from which this proposal stems. As we’ll see, many aspects of the proposal look very good. For example, it seems as though there will be expanded access to healthcare providers outside of NYC for UFT and city employees who live further out. Still, other questions remain unresolved or are answered ambiguously in the FAQs. Without delving into history, it’s a fact that we owe hundreds of millions of dollars in healthcare savings to the City. Those promised savings are going to color how many of us see this plan. Many of us, understandably, will have at least some skepticism. Indeed, some of our first questions, are not answered by the FAQ:
- What percentage of the promised savings are met through this agreement?
- How are those savings met and to what extent (if any) is that done by reducing quality/quantity of care? To what extent (if any) are the savings met by setting the conditions for potential reductions of quality/quantity of care down the line?
- What savings, if any, still need to be met to be in compliance?
- If the answer to the aforementioned question is anything more than 0, what does that mean for how care might change down the line?
So in addition to the obvious questions…
- Based on what we know, what is good about the plan?
- Based on what we know, what is not so good about the plan?
- What don’t we know about the plan that is either good or bad?
…without more information relating to questions 1 and 2, it is impossible to understand whether the new healthcare plan is the only healthcare news we’ll see over the next few months and years or whether new surprises might later transpire. Interestingly, we see some hints of that potential news in the FAQ, which can be accessed by clicking on the link at the bottom of the August 28th email. So, without further ado, after reading the FAQ section (screenshots below), and without being accusatory, we have some thoughts and questions about the new healthcare proposal:
The possibility of tiered hospitals in the future should scare everybody. That would mean that the “better” hospitals would charge higher co-pays, forcing us and our families to go to mid-tier (which would still charge co-pays) or lower-tier (little or no co-pays) hospitals. Besides the obvious disadvantage of not getting the best treatment available, there is also the distinct possibility that the nearest hospital to your home is the one who will charge you an arm and a leg for medical care, should tiered hospitals be implemented down the line.
“We don’t really know if your current doctors will be part of the new city health plan. You should ask them… but they may not know either since they’re not aware of the NYCE PPO.” Perhaps everyone’s doctors will be in-network but this answer leaves a lot to be desired.
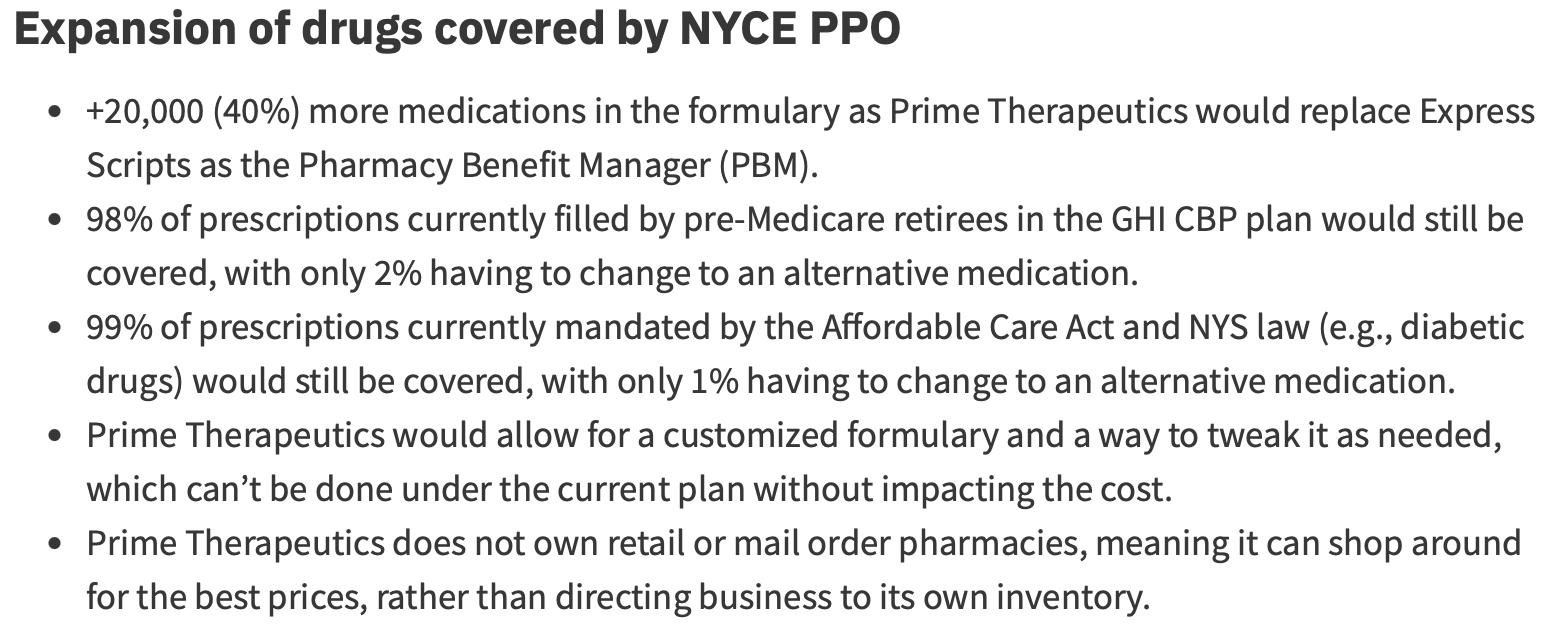
This doesn’t sound terrible, but we would like to know what 2% of prescriptions currently filled by pre-Medicare retirees will have to be changed to an alternative. Same goes for the 1% of prescriptions that are currently mandated by the ACA and NYS law.

The words “not changing at this time” are never comforting, especially when it comes to cancer treatment and injectables.
This is a carefully worded, soft-pedaled definition of prior authorization. What is not mentioned here is the fact that health insurance companies hold our collective fate in the palm of their hand. They can choose to delay or deny procedures on a whim because they profit heavily from doing so (procedures cost them money – if they authorize fewer procedures, they make more money).
We would like some clarification on this. The information is technically not incorrect (i.e. GHI CBP requires prior authorizations for MRIs), but we would like to know, specifically, which procedures and services currently require prior authorizations under GHI CBP, and which procedures and services will require prior authorizations under the proposed NYCE PPO plan.
This sounds like a bunch of gobbledygook. There are no specific timelines given for approvals, denials, or appeals. Right off the bat, it says “The providers would regularly monitor how decisions are made, how quickly the approval process happens, how often care is approved and how well it supports your health care needs.” These are the same providers who make money by delaying and denying treatment.
This sounds like our plan can be altered at any time if the healthcare providers and city aren’t happy with the arrangement. The MLC will be there but a) They’re outnumbered, b) We’ve been stung by them before – will they really defend us from catastrophic changes?, and c) Who would be the arbitrator? We consistently lose arbitration decisions. Currently, the most infamous arbitrator is a power player who has tried to diminish our health insurance for years and has been consistently unfriendly to us.
Which procedures, specifically, will receive fewer denials? There is no wording here that explains which procedures may be denied more frequently under the new plan. Will denials be down all across the board, or will there be an increase in denials in certain areas?
As you can see, although there are some benefits in the new healthcare plan, there are many questions and concerns that have not yet been thoroughly addressed. Hopefully, in the coming weeks, we will get some more clarification. This impacts the vast majority of UFT members and city workers. We need to pay attention and we cannot be afraid to ask questions and voice our thoughts. There can be no ambiguity when it comes to health coverage that protects us and our families.

Thank you for this review and pointed questions. Most important for me was the one about the so called savings to the city. Did the prior agreement between the MLC and the city to push retirees into MA have a specific price tag on the “savings” to the city and is the MLC still on the hook to make good on its promise in other areas like the present plan? This looks like the “pea” in a 3-card monte game.
Shouldn’t members be involved in these negotiations? Do members trust Eric Adams and for-profit health insurance companies acting as third party benefits administrators for a self-funded plan, in which both the City and United Health/Emblem (and the union benefit fund) financially benefit by denying/delaying care to municipal workers and their families? There is a common-sense alternative – now is the time for educators, allying with parents and students, to demand the New York Health Act and reject this new backroom deal: https://thewire.educators.nyc/p/union-members-should-demand-the-new
“They can choose to delay or deny procedures on a whim because they profit heavily from doing so (procedures cost them money – if they authorize fewer procedures, they make more money).”
So, with the transition to the self funded model, this is no longer true. The question becomes how the fee structure for administration is laid out. If they’re paid based on number of approved claims or something like that, then they are incentivized not to deny claims since that would lose them money.
There are still plenty of questions, for example, what will the out of network reimbursement rate be based on? Right now, it’s based on rates from 1983.
Seeing an out of network doctor is just unaffordable with the current plan, and there are some very good doctors who just do not take insurance at all.
For what it’s worth, I started my public service career with the State and was covered by the Empire Plan for years. The Empire Plan is so superior to the GHI CBP in every way imaginable that my husband and I have contemplated just sucking it up and paying the $500 a month to go back to the Empire Plan through his job instead.
The Empire Plan, similar to this new proposed plan, is self funded and administered by UHC. So if the new plan is even half as good as the Empire Plan, it’s going to be a big win. Hopefully it’ll go so well that UFT will give up trying to administer our prescriptions for us… (The UFT prescription plan is hands down the worst I’ve ever encountered. Fingers crossed getting away from Express Scripts will help.)
Definitely plenty of questions still, but I’m cautiously optimistic this change can be good.
keeping track of how the new plan will save the city money will be like a three card monte shell game. With all the unknowns, members have a right to accurate data on how this plan works or doesn’t on our behalf. The UFT has a responsibility to collect member experiences and report back so that patterns and particular issues are identified good and bad.